Circumcision - History and Recent Trends
Circumcision pre-dates recorded history. It has been argued that the practice of circumcision, by freeing the penis of a phimotic foreskin, may have conferred a selective advantage that aided sexual intercourse and thus reproduction, so enhancing the competitive success of our species as it evolved [Cox, 1995; Cox & Morris, 2010]. As such it most likely existed before our species radiated out of Africa 70,000 years ago. This is more plausible than it having arisen independently in different parts of the world. Those cultures that do not currently practice circumcision are most likely to have stopped doing in in more recent times, rather than the other way around. Humans arrived in Australia 50,000 years ago and their paleolithic hunter-gatherer society was maintined until recent times. This included circumcision. Humans most likely evolved as a circumcising species. Those cultures that do not currently circumcise are ones that stopped doing it, not those that did not ever adopt circumcision [Cox & Morris, 2010].
The hypothesis of Cox [Cox, 1995] provides the only consistent explanation for pan-global circumcision traditions. He points out that humans must learn many skills before men and women are self-supporting. Because of this there was a selective advantage in deferring reproduction for quite a while beyond puberty. Those couples who delayed reproduction were likely to have a higher number of offspring who survived, because they were in a better position to support such children. This created an uniquely human paradox - adolescents needed to go through puberty in order to develop the bodily strength required for adult skills, yet it was important for them not to use their biological ability to reproduce during this learning period. Such a situation favoured natural selection of modifications to the genitalia capable of hindering early intercourse. Females developed a hymen and males developed a penis in which the prepuce, by being phimotic, impeded erections and thus successful penetration of the female. Both conditions were painful impediments to first intercourse. But once virginity had been lost they no longer impeded reproduction. So today, in Western Europe, parents commonly intervene to make the foreskins of boys retractable, but in countries where this is not practised, the majority of young adult males suffer from phimosis (see later section on physical problems and phimosis) Once these obstacles have been overcome and intercourse has occurred, the foreskin is redundant and explains why, in adult males, it often does not cover the glans. It thus becomes obvious that circumcision arose (at least in part) as a means of regulating this entire process more precisely. Circumcision was able to define exactly the age at which a male could begin reproduction. This is an excellent explanation of the substantial selective advantage that circumcision conferred. As a consequence those humans who practiced circumcising were better equipped to out-compete those who did not.
So support for circumcision as a cultural imperative is evident from both anatomical and cultural evidence. But there is more support from comparative anatomy, as enunciated in Cox & Morris, 2010 as will now be described.
The penis of humans (Homo) differs considerably from the penis of the other hominids – Pan, Pongo and Gorilla. The fold which forms the foreskin of great apes is attached to the proximal part of the shaft. Therefore, when the foreskin retracts during an erection, most of the penile shaft, the pars medialis, not just the glans, is exposed. In other great apes, the glans itself is less well defined than in Homo. It is most pronounced in Gorilla and not defined at all in Pan (chimpanzees). In the great apes phimosis is unknown, even in infants. Instead, the foreskin is always loose, and retracts with erection. Interestingly, in the orang-utan (Pongo) the glans is exposed in juveniles, but not in adults, which is the complete opposite to what occurs in humans. These observations support the fact that phimosis arose as a specific development in the evolution of the genus Homo. We humans also lost the baculum (penile bone), developed a greater demarcation of the glans, and underwent a repositioning of the foreskin so that there was no longer a pars medialis. Size was another factor. The human penis is much larger than that of Gorilla and while its length is comparable to that seen in Pongo and Pan, it is much larger in diameter. What’s more, it does not retract into the body cavity when flaccid. Some of these modifications are most likely to be related. The loss of the baculum probably goes with the greater diameter and non-retraction of the human penis. It is probable that some changes relate to the changes in the female reproductive tract associated with bipedal locomotion, and the need for the birth canal to permit passage of the much larger human head. Each of these factors mean that a thicker and more flexible penis is advantageous. These factors do not explain, however, the selection pressure for phimosis, nor the rearrangement of the glans and prepuce. The only explanation is the idea that a formal virginity had positive selective value.
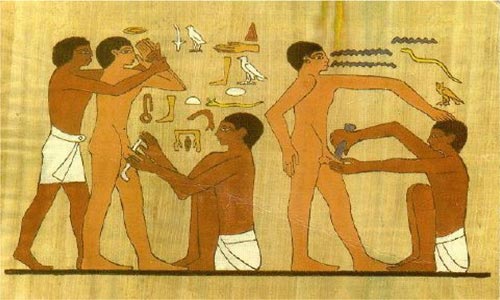
Not only is circumcision one of the oldest, it remains one of the most common, if not the most common, surgical procedure in the world. It is also the subject of interesting anthropological issues [Silverman, 2004]. Egyptian mummies and wall carvings record the practice of circumcision over 4000 years ago [Alanis & Lucidi, 2004]. For example, it is depicted in a wall relief from Saqqara in Lower Egypt, dated about 2300 BC [Szabo & Short, 2000] (see illustration below). The practice appears to have been universal amongst all strata of society in Ancient Egypt [Short, 2006]. A detailed historical evaluation suggests that sound medical reasoning was behind circumcision becoming a religious custom in ancient Egyptian civilization [Spigelman, 1997]. It was usually performed by priests in late puberty to all boys [Cox & Morris 2018]”.
There is evidence to suggest that hygiene may be another reason for circumcision. This appears to be the case for elite classes in ancient Egypt and the Aztec peoples [Remondino, 1891]. It has, moreover, been suggested that the practise of circumcision by indigenous populations in the hot, dry, sandy environments of the deserts of Egypt, Saudi Arabia, Mexico, the Kalahari and central Australia may have been a practical solution to the fact that sand would readily get under the foreskin and set up balanitis, which could lead to urethritis, cystitis, nephritis and death [Short, 2006].
Ritualistic circumcision has been practiced in West Africa for more than 5000 years and in the Middle East for over 4000 years [Warner & Strashin, 1981; Moses et al., 1998]. It is virtually universal in the Jewish and Muslim religions, having started with Abraham (Genesis 17: 11) who lived around 2000 BC. Abraham was unable to get Sarah (his wife) pregnant. At an advanced age we are told that God ordered him to get circumcised, and he promptly succeeded in fathering a son, Isaac, by Sarah. The ages of the people concerned cannot be reported correctly – probably through a mistranslation of some ancient time unit such as ‘seasons’ into years. A scholarly evaluation of various passages in the Bible suggests that certain ages stated were twice the true age. Thus Abraham was 50 and Sarah was 45. She probably thought she had reached menopause, but as many women have found, menopause is not an “on-off switch”. Sarah was still attractive enough at 45 for the king Abimilech to want her as his wife – an implausible notion if she were 90. As soon as Abraham was circumcised, he was able to get Sarah pregnant, so his problem was clearly phimosis. Abraham then had all in his household circumcised. All of this suggests strongly that they were living among people to whom circumcison was a familiar operation. 40 years later, when the Israelites under Joshua reach the Promised Land, circumcison had died out, and God issued them with specific instructions about making stone knives, which in those days were much sharper than the bronze knives in everyday use.
Not all populations at the time retained circumcision. The Bible states that the Philistines (Palestinians) were uncircumcised. By 500 BC, however, Herodotus reported that they were circumcised [Cox & Morris, 2010]. The Syrians too were said to have once been uncircumcised, but later adopted it from the Egyptians. This adds to the view that circumcision was current across North Africa and Asia Minor in pre-Islamic times.
Circumcision is a univeral practice of Muslims, even though it is not mentioned in the Qu’ran. Circumcision is a matter of cleanliness and hygiene, and was already universal in the time of the prophet Mahommad. Islam lays great stress on matters of cleanliness, not just ritual cleanliness but the everyday practical form as well, to a far greater degree than other major religions. A 15th century Ottoman textbook describes the procedure in detail [Kendirci et al., 2005]. Although some urban Muslims these days have adopted neonatal circumcision, the commonest practice has been to circumcise boys between the ages of 4 and 10. It is an important festive event, at which the boy wears special, elaborate clothing and receives many presents. It is therefore no surprise that it is a keenly-awaited occasion for the boy.
In the non-Muslim African countries of Cameroon and the Congo most men are circumcised. Similarly, in Kenya (mostly non-Muslim) all tribes except the Luo practice male circumcision. This no doubt reflects practice dating back 80,000 years when modern humans evolved.
At some stage the inhabitants of Europe, who were circumcised in Palaeolithic times, abandoned the practice. The most likely explanation is that at a time of extreme privation, perhaps during a glacial period, ritual life was lost in the struggle for survival [Cox & Morris, 2010]. One can draw a parallel with the loss of the tradition among the Jewish people during the time of their wanderings and starvation in the wilderness. In contrast to Europe pre-history, in north Africa and Asia Minor the warmer climate spared the population such traumas and so ritual life continued, leading in time to the world’s first advanced, literate civilizations [Cox & Morris, 2010].
Along with Columbus' 'discovery' of North America he noted that many of the natives there were circumcised [Gairdner, 1949]. The advanced civilizations of pre-Columbian America practised circumcision, although the more primitive tribal people did not. Once again, this may reflect the loss of ritual in times of privation. The Spanish conquistadores banned the practice as part of their systematic destruction of the indigenous cultures. It is now rare in South America, though more common in Latin North America.
In the late 19th century circumcision became routine in the United States of America and elsewhere as a result of pronouncements in publications by various physicians, most notably Peter Remondino [Remondino, 1891; Gollaher, 1994; Alanis & Lucidi, 2004]. He recognized the various health benefits at the time, although he overemphasized the clinical significance of the foreskin in masturbation, a practice thought at the time to have adverse consequences [Schoen, 2007d]. Most other authorities at the time did not agree with him on this point, as is discussed in the next paragraph. The procedure rapidly gained popularity and became routine.
Some of the purported benefits have stood the test of time, namely that circumcision prevents penile cancer, syphilis, balanoposthitis and phimosis. Although it is often claimed (by anti-circumcision activists) that circumcision was popular in the Victorian era as a cure for masturbation, the truth is quite different. This hypothesis appeared in an 1891 commentary [Hutchinson, 1891] by an author who, decades earlier, was the first to observe that circumcision protects against syphilis [Hutchinson, 1855]. But the idea that circumcision prevented masturbation had no common currency in Victorian times. For example, the purported 'evil' of masturbation occupies much of the 1913 book 'Youth and Sex', yet circumcision is not mentioned [Scharlieb & Silby, 1913]. A well-known book on circumcision by Felix Bryke completely rubbishes the idea [Bryk, 1934] and Whitla's 'Dictionary of Treatment' does not list 'circumcision', whereas, under 'masturbation, only suggests performing circumcision if irritation from a tight prepuce is responsible [Whitla, 1912].
Benefits of circumcision espoused in Victorian times included protection against syphilis [Hutchinson, 1855], other STIs [Anonymous, 1874], phimosis [Anonymous, 1874; Sayre 1888], paraphimosis [Anonymous, 1874], balanitis [Anonymous, 1874], preputial adhesions [Sayre, 1888], inferior hygiene [Anonymous, 1874], and cancer [Hutchinson, 1890]. These benefits appeared in early 20th century publications as well [Freeland, 1900; Wolbarst, 1914; Silby, 1913].
By the mid-1930s about half of male newborns in the USA were circumcised, and increased to about 90% in the 1950s and 1960s (after World War II when the Armed Forces demonstrated the health advantages [Culp & Patton, 1987; Patton, 1987b; Patton, 1987a; Stewart, 1987; Vermooten, 1987]). In the early 1970s promotion of infant bonding became popular, and ways of reducing discomfort in newborns were advocated, leading some middle-class families on the East and West coast of the USA to not get their boys circumcised. The folly of this became evident as research unfolded over the years, as will be discussed in this internet review, and the rate of circumcision then rose between 1988 and 2000 [Nelson et al., 2005; Schoen, 2005a].
The British Royal family has a tradition of circumcision, there being no doubt whatsoever that Prince Charles was circumcised by Dr Jacob Snowman, who was also a Jewish mohel (ritual circumciser). Circumcision was a common practice among the British middle and wealthy classes from the 1890s to at least the 1940s. Research showing protection against syphilis, penile cancer and the improvement in hygiene led to it becoming a widely recommended for hygienic and health reasons. Not surprisingly, the British Royal family followed this “new” fashion. The medical wisdom of the day tends to support the probability that Royals from George V through to Prince Charles and his brothers were circumcised. As for the sons of Dianna and Charles, Palace insiders attest to Princes William and Harry being circumcised, whereas some others claim that because Dianna was opposed they did not receive a circumcision. There is no hard evidence either way. Nevertheless, many a young lady will know from first hand experience the answer to this question. As far as the circumcision custom of the British royals are concerned, a biography of the young princes by the very well informed Ms Ingrid Seward (http://books.google.hu/books?id=XBSnAgAAQBAJ&hl=hu&source=gbs_%20similarbooks) confirms (p 33) that the boys were indeed circumcised at birth. Given the fact the Duchess of Cambridge's father's side is a well-to-do upper middle class of several generations of solicitors (http://en.wikipedia.org/wiki/Family_of_Catherine,_Duchess_of_Cambri_dge), with an upwardly mobile and very ambitious mother, it is very probable that both Michael Middleton, the father of Kate, and James Middleton, her brother, are both circumcised. As for the young Prince George and Prince Louis, while some suspect that they were circumcised, there is no certainty as yet. The newly granted Middleton family arms depicts 3 acorns: http://en.wikipedia.org/wiki/Family_of_Catherine,_Duchess_of_Cambridge#Arms ... Is there a message in this?
In the United Kingdom, most consider that a trend not to circumcise started in 1948 when Britain adopted a nationalized healthcare system and removed procedures in which it considered cost exceeded benefit. But unpublished data by Waskett & Morris suggests rates had started to fall in the 1930s. Circumcision also dropped rapidly across Europe after a (misguided) paper by Gairdner in 1949 [Gairdner, 1949].
It was not until the early 1970s that a similar fall happened in Australia and Canada, in response to statements by the pediatric bodies in each country [Australian, 1971; Committee., 1975].
Trends across Asia are mixed and complex. Hinduism prohibits circumcision, even any interference with a tight foreskin. Sikhism, which arose more recently, specifically bans circumcision in its holy book, which dates from 1708. It is clear from the context that this is a reflection of its rejection of Islamic customs. Buddhists do not circumcise, though this seems to be more of a philosophical tradition of not inflicting harm than a specific prohibition. The original inhabitants of Japan, the Ainu, practised circumcision, but the modern Japanese (of Korean descent) do not [Cox & Morris, 2010]. Whether this is the result of ethnic traditions or of the Buddhist religion is not clear.
In India and China circumcision was not practised, presumably as a result of Hindu and Buddhist influence. Circumcision was once customary in Sulawesi, and therefore probably throughout the Indonesian archipelago. The spread of Buddhism and Hinduism into the regions led to the abandonment of circumcision, but it later became the norm again following the adoption of Islam. Islam also brought circumcision to much of the Indian sub-continent. Aboriginal Taiwanese practice circumcision, like their ethnic cousins the Filipinos, but successive Chinese invasions of the island in the last 400 years have made these Taiwanese a minority [Cox & Morris, 2010].
Thus circumcision is seen in diverse people all over the world, ranging from African, Middle Eastern, groupings within Asians, Australian aboriginals, Pacific Islanders and native Americans, both North and South. This indicates a very ancient origin that was part of human practice as our species colonized the globe, rather than it having arisen independently in different regions of the world. By historic times circumcision had entirely lost its original significance of permitting marriage, and had become a badge of cultural and/or religious identity, so that changes in circumcision status reflected changes in cultural or religious affiliations. The promotion of circumcision because of its benefits to health has re-emerged as the primary underlying theme in the era of modern medicine.



